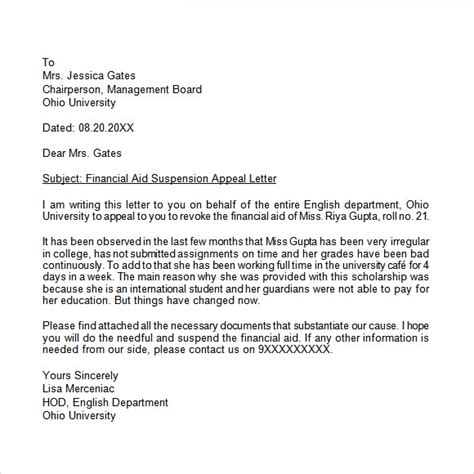
Letter Of Appeal Sample Format. Authorization for treatment with [medication] dear medical or pharmacy director: Instructions for a letter of appeal:

You will notice that the text of this sample letter is exceptionally brief. [ your name] [ your position, if relevant] [ your address] [ your phone number] [ your email] Use the following template to help you write your letter: